Understanding Modern Minimally Invasive Spine Fusion Techniques
Spinal fusion surgery has evolved significantly over the years, with modern minimally invasive techniques aiming to provide effective spinal stabilization while reducing tissue damage, postoperative pain, and recovery time.
Two advanced fusion techniques commonly discussed today include:
· UBE-TLIF (Unilateral Biportal Endoscopic – Transforaminal Lumbar Interbody Fusion)
· OLIF (Oblique Lumbar Interbody Fusion)
Both are modern minimally invasive fusion procedures designed to treat selected spinal conditions such as instability, degeneration, stenosis, and deformity.
Importantly:
No single technique is best for every patient.
The most appropriate surgical approach depends on:
· Type of spinal pathology
· Degree of instability
· Patient anatomy
· Nerve compression pattern
· Bone quality
· Number of spinal levels involved
· Surgeon expertise and experience
· Overall patient health and recovery goals
The primary focus should always remain on safe, evidence-based, and individualized patient care.
What is UBE-TLIF?
UBE-TLIF stands for:
UBE
Unilateral Biportal Endoscopy
TLIF
Transforaminal Lumbar Interbody Fusion
UBE-TLIF is an advanced minimally invasive fusion procedure performed using:
· One portal for the endoscopic camera
· One portal for surgical instruments
The surgery is performed from the back of the spine using a transforaminal pathway.
The procedure may involve:
· Nerve decompression
· Removal of damaged disc material
· Placement of a fusion cage
· Bone grafting
· Pedicle screw stabilization
UBE-TLIF combines spinal fusion principles with modern endoscopic technology and is increasingly recognized as part of:
“4th Generation Endoscopic Spine Surgery”
What is OLIF?
OLIF stands for:
Oblique Lumbar Interbody Fusion
OLIF is a minimally invasive fusion procedure performed through an oblique side approach to the spine.
Instead of approaching the spine directly from the back, OLIF accesses the disc space through the side of the abdomen using a natural tissue corridor.
The procedure typically involves:
· Disc removal
· Placement of a large fusion cage
· Restoration of disc height
· Indirect nerve decompression
· Supplemental stabilization when required
OLIF is widely used for selected degenerative and deformity-related spinal conditions.
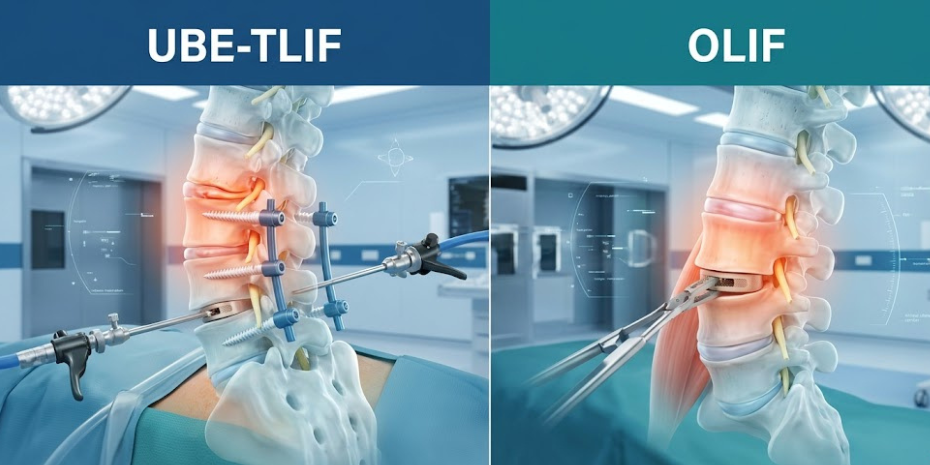
Major Difference Between UBE-TLIF & OLIF
UBE-TLIF
· Posterior (back) approach
· Endoscopic biportal technique
· Direct nerve decompression
· Familiar posterior spinal anatomy
· Fusion through transforaminal access
OLIF
· Side (oblique lateral) approach
· Access through retroperitoneal corridor
· Indirect decompression through disc height restoration
· Larger cage placement possible
· Reduced posterior muscle disruption in selected cases
Both techniques are valuable and have different strengths depending on the spinal condition being treated.
How Nerve Decompression Differs
UBE-TLIF
UBE-TLIF allows:
· Direct visualization of nerves
· Direct decompression of stenosis
· Removal of compressive structures under endoscopic guidance
This may be particularly useful in:
· Severe lumbar canal stenosis
· Foraminal stenosis
· Complex nerve compression
· Revision decompression cases
OLIF
OLIF often works through:
Indirect Decompression
By restoring disc height and spinal alignment, pressure on nerves may reduce indirectly without directly exposing the spinal canal.
In selected patients, this can provide excellent symptom relief with less posterior tissue disruption.
However, some patients may still require additional posterior decompression procedures depending on the severity of stenosis.
Surgical Access & Anatomy
UBE-TLIF
· Performed through small posterior portals
· Uses endoscopic visualization
· Allows direct access to posterior spinal structures
OLIF
· Approaches the spine from the side
· Avoids major posterior muscle dissection
· Works through the retroperitoneal corridor near abdominal structures
Each approach has specific anatomical considerations and technical requirements.
Conditions Commonly Treated
UBE-TLIF May Commonly Be Used For
· Lumbar instability
· Recurrent slipped disc
· Lumbar canal stenosis
· Foraminal stenosis
· Degenerative disc disease
· Spondylolisthesis
· Revision spine surgery in selected cases
OLIF May Commonly Be Used For
· Degenerative disc disease
· Spinal alignment correction
· Adult degenerative scoliosis
· Multi-level degeneration
· Selected instability cases
· Disc height restoration procedures
Again, the ideal procedure depends on the patient’s individual pathology and surgical goals.
Visualization & Surgical Technique
UBE-TLIF
Provides:
· Magnified endoscopic visualization
· Continuous irrigation
· Independent instrument movement
· Direct decompression capability
OLIF
Provides:
· Large disc space access
· Placement of larger interbody cages
· Indirect decompression potential
· Alignment restoration advantages in selected cases
Both procedures require specialized training and surgical expertise.
Benefits of UBE-TLIF
Potential Advantages
· Direct nerve decompression
· Minimally invasive biportal approach
· Reduced muscle damage
· Smaller incisions
· Early mobilization
· Advanced endoscopic visualization
· Useful in selected revision cases
Benefits of OLIF
Potential Advantages
· Avoids posterior muscle dissection
· Large cage placement capability
· Disc height restoration
· Alignment correction potential
· Useful for selected multi-level procedures
Risks & Limitations
All spinal fusion surgeries carry potential risks regardless of technique.
Possible Risks Include
· Infection
· Bleeding
· Persistent pain
· Nerve irritation or injury
· Implant-related complications
· Dural tear (CSF leak)
· Non-union or delayed fusion
· Recurrent symptoms
Specific Considerations in UBE-TLIF
Potential challenges may include:
· Technical learning curve
· Endoscopic surgical complexity
· Limited suitability in severe deformity cases
Specific Considerations in OLIF
Potential challenges may include:
· Vascular or abdominal structure proximity
· Indirect decompression limitations in severe stenosis
· Need for supplemental posterior fixation in selected cases
Proper patient selection remains critical for both techniques.
Which Technique is Better?
The Most Important Principle:
The best procedure is the one most appropriate for the individual patient.
There is no universally “superior” fusion technique for every spinal condition.
The final decision depends on:
· MRI findings
· Instability severity
· Alignment goals
· Nerve compression pattern
· Bone anatomy
· Number of spinal levels involved
· Patient health status
· Surgeon expertise and experience
Both UBE-TLIF and OLIF are valuable modern fusion procedures when used in appropriately selected patients.
Recovery After UBE-TLIF & OLIF
Recovery varies depending on:
· Number of spinal levels treated
· Degree of instability
· Patient health condition
· Bone quality
· Rehabilitation progress
General Recovery Expectations
Early Phase
· Walking often begins within 24–48 hours
First Few Weeks
· Gradual increase in mobility
· Pain reduction
· Light activity progression
Long-Term Recovery
· Fusion healing continues over months
· Physiotherapy and strengthening remain important
Both procedures aim to support earlier mobilization compared to traditional open fusion surgery.
Frequently Asked Questions
Is UBE-TLIF Better Than OLIF?
Neither technique is universally better for every patient. The correct procedure depends on pathology, anatomy, instability, and surgical goals.
Which Procedure Has Smaller Incisions?
Both are minimally invasive procedures using smaller incisions compared to traditional open fusion surgery.
Does OLIF Avoid Back Muscles?
OLIF approaches the spine from the side and may reduce posterior muscle disruption in selected patients.
Does UBE-TLIF Provide Direct Nerve Decompression?
Yes. UBE-TLIF allows direct endoscopic decompression of nerves and spinal stenosis.
Can Both Procedures Treat Instability?
Yes. Both techniques are used for selected spinal instability and degenerative conditions.
Is Recovery Faster Than Open Fusion Surgery?
Many patients experience reduced tissue trauma and faster mobilization compared to traditional open surgery.
How is the Final Surgical Decision Made?
The decision is based on clinical examination, MRI findings, spinal stability, anatomy, alignment goals, and surgeon expertise.
Ethical & Evidence-Based Spine Care
Modern spine surgery should never focus on promoting one technique for every patient.
The priority should always be:
· Accurate diagnosis
· Individualized treatment planning
· Conservative treatment whenever appropriate
· Evidence-based decision-making
· Safe minimally invasive techniques when suitable
Different spinal conditions require different surgical strategies.
The goal is always to select the most appropriate treatment for long-term patient benefit.
Book a Consultation for Minimally Invasive Spine Fusion
If you are suffering from spinal instability, recurrent slipped disc, lumbar canal stenosis, or chronic nerve compression symptoms, expert evaluation can help determine which minimally invasive fusion approach may be most appropriate for your condition.
Schedule Your Appointment Today
· MRI Review
· Spine Stability Evaluation
· UBE-TLIF Consultation
· OLIF Consultation
· Second Opinion for Spine Surgery
· Personalized Treatment Planning