Understanding the Difference Between Two Advanced Minimally Invasive Spine Surgery Techniques
Modern spine surgery has evolved significantly over the last two decades. Today, many spinal conditions can be treated using minimally invasive techniques that aim to reduce tissue damage, improve recovery, and preserve normal spinal structures.
Two commonly discussed advanced minimally invasive approaches are:
UBE (Unilateral Biportal Endoscopic) Spine Surgery
Tubular Minimally Invasive Spine Surgery (Tubular MIS Surgery)
Both techniques are valuable and effective when used in appropriately selected patients.
Importantly:
No single technique is best for every patient.
The correct surgical approach depends on:
Type of spinal pathology
Location of nerve compression
Presence of spinal instability
Patient anatomy
Severity of degeneration
Previous surgeries
Surgeon expertise and experience
Overall patient health
The goal should always be to choose the safest and most effective treatment for the individual patient — not simply the newest technology.
What is UBE Spine Surgery?
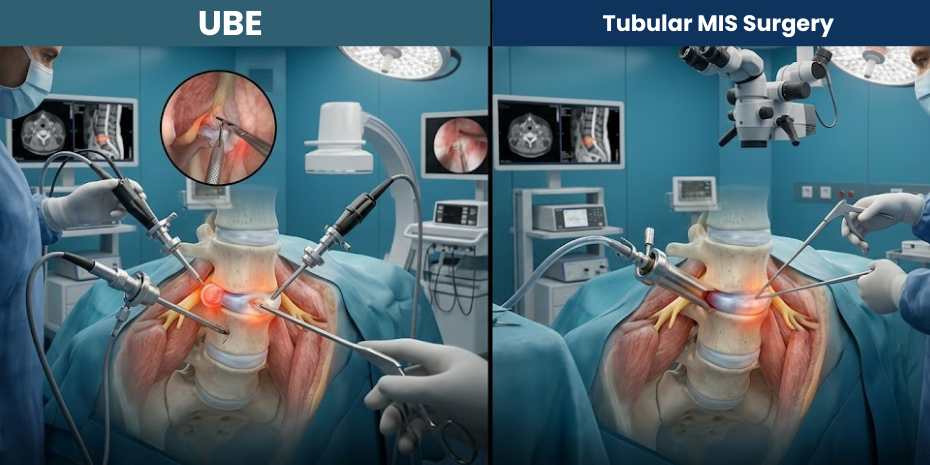
UBE (Unilateral Biportal Endoscopic) Spine Surgery is an advanced minimally invasive technique that uses:
One small portal for the endoscopic camera
One small portal for surgical instruments
The endoscopic camera provides magnified, illuminated visualization of the spine, while the separate working portal allows greater instrument flexibility.
UBE is increasingly recognized as part of the evolution toward 4th Generation Endoscopic Spine Surgery.
Common Uses of UBE
Slipped disc
Sciatica
Lumbar canal stenosis
Endoscopic decompression
Selected fusion procedures (UBE-TLIF)
Certain revision spine surgery cases
What is Tubular MIS Surgery?
Tubular Minimally Invasive Spine Surgery uses specialized tubular retractors to create a small pathway through the muscles to the spine.
The surgery is typically performed using:
An operating microscope
Surgical loupes
Specialized minimally invasive instruments
Instead of large muscle dissection, the muscles are gently dilated and separated using tubular systems.
Common Uses of Tubular MIS Surgery
Microscopic discectomy
Lumbar decompression
Minimally invasive fusion surgery
Selected cervical and lumbar procedures
Certain spinal stabilization surgeries
Tubular surgery represented a major advancement over traditional open spine surgery and continues to be widely used worldwide.
UBE vs Tubular MIS Surgery: Key Differences
Visualization
UBE
Uses a high-definition endoscopic camera inside the surgical field, providing magnified and illuminated visualization.
Tubular MIS
Usually relies on a microscope positioned outside the body.
Surgical Access
UBE
Uses two separate portals:
Camera portal
Instrument portal
This allows independent instrument movement.
Tubular MIS
Uses a tubular retractor system through a single working channel.
Instrument Flexibility
UBE
The biportal design often allows greater freedom of instrument movement and wider decompression capability.
Tubular MIS
Instrumentation works through a fixed tubular corridor.
Tissue Preservation
Both techniques are designed to minimize muscle injury compared to traditional open surgery.
Both aim to preserve normal spinal structures as much as possible.
Learning Curve
UBE
Requires specialized endoscopic training and familiarity with biportal visualization.
Tubular MIS
Requires expertise in microscopic minimally invasive surgery and tubular access techniques.
Both procedures require significant surgical experience for optimal outcomes.
Advantages of UBE Spine Surgery
Potential Benefits
Excellent endoscopic visualization
Magnified surgical field
Smaller skin incisions
Reduced muscle trauma
Good decompression capability
Early mobilization
Faster recovery in selected patients
Useful in certain revision cases
Advanced minimally invasive fusion possibilities (UBE-TLIF)
Advantages of Tubular MIS Surgery
Potential Benefits
Proven and widely established technique
Smaller incisions compared to open surgery
Reduced muscle damage
Effective microscopic decompression
Strong role in minimally invasive fusion surgery
Familiar anatomy for many spine surgeons
Excellent results in appropriately selected patients
Are There Situations Where One Technique May Be Preferred?
Yes. The ideal technique depends on the spinal condition being treated.
UBE May Be Particularly Useful In
Lumbar canal stenosis
Wide decompression requirements
Certain revision surgeries
Selected endoscopic fusion procedures
Patients seeking advanced endoscopic options
Tubular MIS May Be Particularly Useful In
Focused disc surgery
Certain stabilization procedures
Microscopic decompression
Specific fusion techniques
Cases where tubular access offers efficient treatment
However, these are not rigid rules.
The best surgical plan should always be individualized.
Which Technique is Less Invasive?
Both UBE and Tubular MIS are considered minimally invasive spine surgery techniques.
Compared to traditional open surgery, both aim to:
Reduce tissue disruption
Minimize muscle injury
Lower blood loss
Improve recovery
Enable earlier mobilization
The actual invasiveness depends on:
Surgical complexity
Number of spinal levels
Patient anatomy
Extent of pathology
Recovery After UBE vs Tubular MIS Surgery
Recovery timelines vary depending on:
Procedure type
Severity of spinal disease
Nerve compression duration
Fusion vs non-fusion surgery
Patient health condition
General Recovery Expectations
Same Day / Next Day
Walking often begins early
1–2 Weeks
Reduction in surgical discomfort
Light activity resumed
2–6 Weeks
Gradual return to routine activities
6–12 Weeks
Rehabilitation and strengthening continue
Both techniques are designed to support faster recovery compared to traditional open surgery in selected patients.
Risks & Limitations
All spine surgeries — including UBE and Tubular MIS — carry potential risks.
Possible Risks Include
Infection
Bleeding
Persistent pain
Nerve irritation or injury
Dural tear (CSF leak)
Recurrent symptoms
Incomplete symptom relief
Not every patient is suitable for minimally invasive surgery.
Certain complex conditions may still require traditional open procedures.
The Most Important Question: Which Technique is Right for You?
The answer depends on:
MRI findings
Clinical symptoms
Presence of instability
Severity of stenosis
Disc pathology
Previous surgery
Bone quality
Overall medical condition
Most importantly, treatment should be individualized.
The best surgery is not defined by marketing terms.
It is defined by:
Correct diagnosis
Appropriate patient selection
Surgical precision
Evidence-based decision-making
Long-term functional outcome
Ethical & Evidence-Based Spine Care
Modern spine care should never focus on promoting one technique for every patient.
Instead, treatment should prioritize:
Patient safety
Accurate diagnosis
Conservative care whenever appropriate
Personalized surgical planning
Choosing the right technique for the right patient
An experienced spine surgeon should be able to recommend the most appropriate option based on the individual clinical situation.
Frequently Asked Questions
Is UBE Better Than Tubular MIS Surgery?
No single technique is universally superior. Both are advanced minimally invasive approaches with their own strengths and ideal indications.
Is Recovery Faster with UBE?
Many patients recover quickly after UBE surgery, but recovery also depends on the underlying condition and type of procedure performed.
Does Tubular MIS Surgery Still Have an Important Role?
Yes. Tubular minimally invasive surgery remains a highly valuable and widely used spine surgery technique.
Which Procedure Causes Less Muscle Damage?
Both techniques are designed to minimize muscle injury compared to traditional open surgery.
Can Both Techniques Be Used for Slipped Disc?
Yes. Both UBE and Tubular MIS techniques can effectively treat selected slipped disc cases.
Which Technique is Better for Lumbar Canal Stenosis?
Both techniques may be used depending on the extent and pattern of stenosis, surgeon experience, and patient anatomy.